Anatomy & function
There are two menisci in every knee joint: the inner men iscus and the outer meniscus. These are two crescent-shaped cartilage discs that serve as stabilisers, shock absorbers, pressure distributors and brake pads, among other things. They also compensate for unevenness between the bones that form the joint. The medial meniscus is fused to the medial collateral ligament of the knee and can therefore hardly give way during a jerky movement. This is the reason why the medial meniscus is much more susceptible to injury and more frequently affected by tears than the lateral meniscus. In addition, the medial meniscus absorbs up to 50% of the pressure of the knee joint, which gives the medial meniscus an additional increased susceptibility to meniscal injury.
You are currently viewing a placeholder content from Spotify. To access the actual content, click the button below. Please note that doing so will share data with third-party providers.
More Information '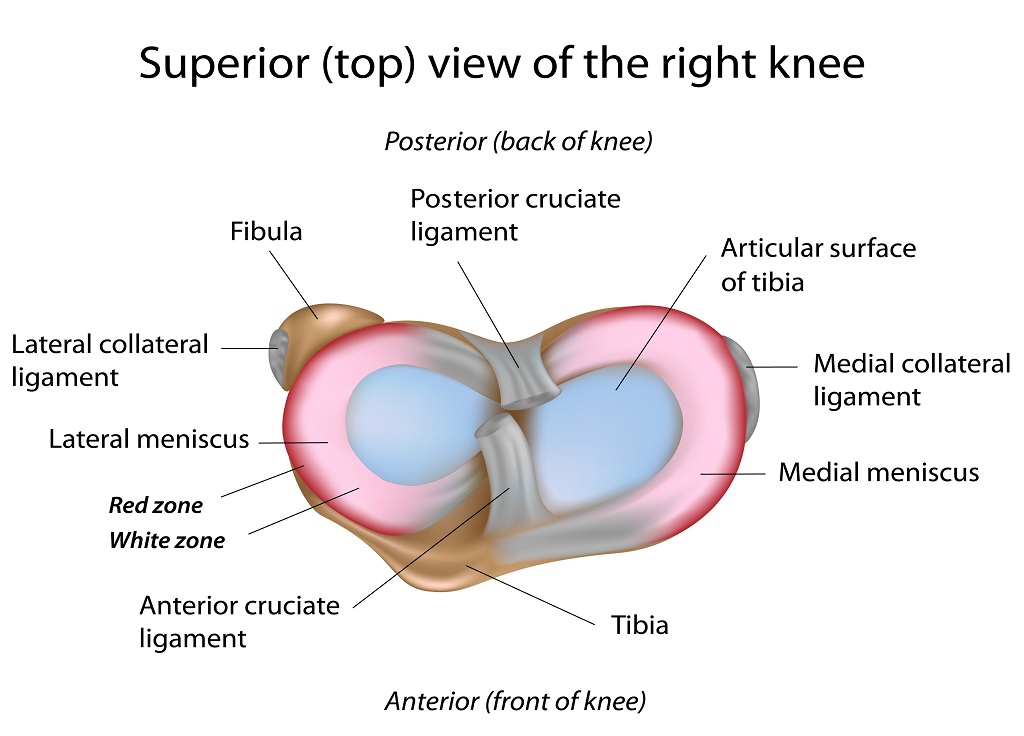
Symptoms & complaints
Whether and to what extent symptoms appear in the case of a meniscus tear depends on the one hand on whether the tear was caused by an accident or by wear and tear.
Signs of a meniscus tear can be
- Knee pain (acute or gradual)
- Effusion in the knee joint
- Swellings
- Impairment of mobility
- Reduction of the load capacity
- Pinching symptoms
- Feeling of instability
- Irritation and inflammation
Causes
Lay people know the meniscus tear as a typical sports injury. What many do not know: Wear and tear can also cause damage to the cartilage tissue and lead to tears.
Causes of a meniscus tear include:
- An injury / twisting of the knee under load, e.g. in the context of a sports injury, often in conjunction with a cruciate ligament injury.
- Thesmallest injuries (microtraumas), during certain movements, e.g. constant bending loads on the knee joint.
- Signs of wear and tear in the meniscus tissue due to age-related overloading, leg axis malpositions, cartilage damage and/or instabilities mostly as a result of anterior cruciate ligament injuries.
Diagnosis
More information will follow shortly.
Treatment
Various therapy components can be considered for the treatment of meniscus tears. Which ones are used depends, among other things, on how severe the pain and suffering of the affected person are and whether the mobility of the joint is impaired. Last but not least, the age of the patient also plays a role, for example, in the question of whether meniscus surgery is necessary.
Conservative therapy
Basically, meniscus tear treatment aims to relieve or eliminate the pain and restore the mobility and resilience of the knee joint.
The following therapies are possible:
- Medicinaltreatment: Medicinal meniscus tear treatment aims to relieve the pain or make it disappear completely
- Physiotherapy: Physiotherapy - special exercises to strengthen the muscles and mobilise them.
- Physical measures: e.g. electrotherapy , cold treatment
- Aids: e.g. walkingaids, knee supports, orthoses
Operation
If the conservative treatment does not result in an improvement of the pain and the continued restriction of movement and weight-bearing, surgical removal of the meniscus damage is recommended. All surgical procedures can usually be performed arthroscopically, minimally invasive, by means of arthroscopy.
Meniscus resection (partial meniscus removal)
At the beginning of the meniscus operation, an arthroscopy is first performed. This procedure allows the surgeon to gain an insight into possible damage to the menisci. Arthroscopy is often necessary because even state-of-the-art diagnostic procedures such as the use of magnetic resonance imaging (MRI) may not always allow a reliable diagnosis. Partial meniscus removal is the most frequently used surgical measure when preservation of the meniscus is not possible.
A standard procedure for the surgical treatment of degenerative or non-refixable meniscal damage is arthroscopic partial men iscectomy - this surgical method for the therapy of meniscal damage is based on the principle of removing only the damaged meniscal tissue. With this surgical procedure, at least 50% of the meniscus substance remains and the fibrous ring can also be preserved. The essential advantage of this therapeutic measure is faster rehabilitation, less postoperative effusion formation and the reduced probability of developing arthrosis of the joint.
Everything at a glance:
- Operating time: 15-30 min.
- Anaesthesia: General spinal local
- Hospital stay: outpatient and inpatient
- Fit for work: 2-4 weeks
- return to sports (RTS): 6-8 weeks
Meniscus suture (meniscus reconstruction)
This method is a minimally invasive procedure in which the damaged meniscus is fixed to the bone structure of the knee joint using a suture material. Meniscus refixation is the gold standard (optimal therapy option) for meniscus damage, but this therapy can only be used for certain tears or tearing of the capsule, as only with this type of damage can the meniscus be reattached and the meniscus damage fully healed.
Meniscus root reconstruction (transosseous meniscus root fixation)
This method is also a minimally invasive procedure with which the inner or outer meniscus, which has been torn off at the bony attachment - usually in the posterior horn - is reattached with a transosseous pull-out suture. Root injuries are considered to be a particularly serious meniscus injury because they can almost completely eliminate the function of the meniscus. Due to the serious consequences of this injury and the only unsatisfactory results after conservative therapy, arthroscopic refixation of the meniscus root by means of a transosseous pull-out suture is now considered the therapy of choice.
Meniscus ramp lesion
Meniscosynovial lesions (MSL or ramp lesions) are often associated with injuries to the anterior cruciate ligament (ACL). They can only be diagnosed to a limited extent during routine knee arthroscopy and also in radiological diagnostics. The clinical relevance of these lesions has not yet been clearly clarified. However, they are often associated with early failure of ACL replacements. Inspection of the posteromedial knee joint compartment in arthroscopically confirmed ACL injury via the trans-notch portal and examination of the meniscocapsular structures with the palpation hook via a posteromedial working portal should be routinely performed. If MSL is diagnosed, repair contributes to a significant improvement in knee joint laxity and thus possibly to better long-term results if ACL replacement surgery is performed at the same time. The reconstruction of the posteromedial structures is technically demanding and is performed arthroscopically via one or two posteromedial working portals.
Everything at a glance:
- Operating time: 30-45 min.
- Anaesthesia: general/spinal/local
- Hospital stay: outpatient and inpatient
- Fit for work: after 4-8 weeks
- return to sports (RTS): 10-12 weeks
Meniscus replacement (meniscus transplantation)
If the meniscus has usually been completely removed in a young person, there is the possibility of a meniscus transplant or a meniscus replacement. Meniscus replacement surgery serves to delay the development of osteoarthritis and is tied to certain anatomical conditions, e.g. the existing cartilage should be undamaged, intact ligamentous conditions should be present and the leg axis should be straight. A transplantation of a donor meniscus ("allograft") is possible as well as the implantation of artificially produced meniscus replacement tissue. After implantation of the meniscus replacement tissue, a long healing period of several weeks is required. Due to the very strict indication, this form of meniscus surgery is performed less frequently overall. There is also a lack of scientific studies that clearly prove the effectiveness of this method.
Aftercare
The result of a meniscus operation depends not least on the special rehabilitation measures carried out. Depending on the type of operation, the knee can be used again immediately or must be rested for a while. With the "Meniscus surgery treatment calendar" we provide you with a treatment schedule from the day of the operation until you return to sporting activities or everyday work, in order to enable an individual, optimised and coordinated treatment sequence.
Meniscus removal treatment calendar
Your treatment roadmap after meniscus surgery. An individualised aftercare concept for arthroscopic meniscus removal surgery.
→ Treatment calendar meniscus removal
Treatment calendar meniscus suture
Your treatment roadmap after meniscus surgery. An individualised aftercare concept for arthroscopic meniscus suture surgery.
FAQs
More information will follow shortly.

