You are currently viewing a placeholder content from YouTube. To access the actual content, click the button below. Please note that doing so will share data with third-party providers.
More InformationAnatomy & function
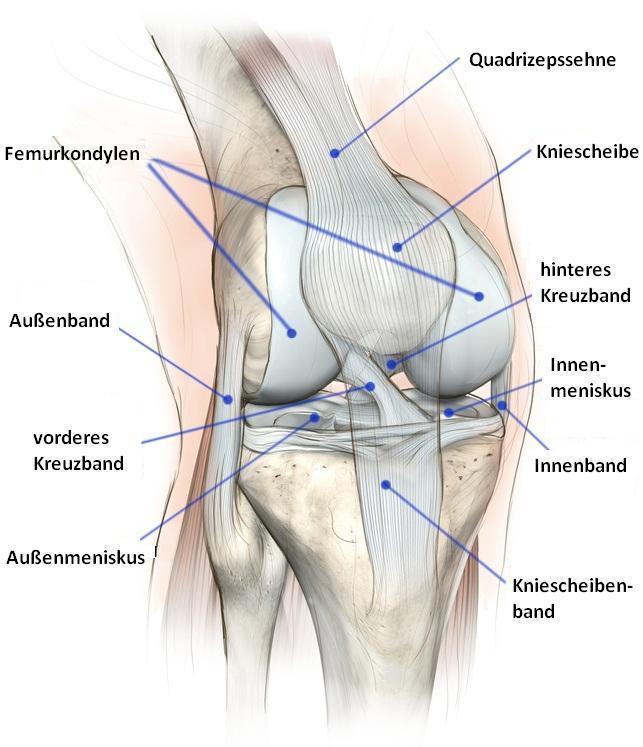
The knee joint connects the upper and lower leg bones and the kneecap. The ends of the bones and the inside of the kneecap are covered with cartilage. Healthy cartilage is a smooth gliding surface that allows low-friction movement in the joint. Osteoarthritis occurs when the cartilage softens, cracks and becomes thinner. Cartilage cannot regenerate as well as other tissues. Once major damage has occurred, it therefore remains.
What is osteoarthritis?
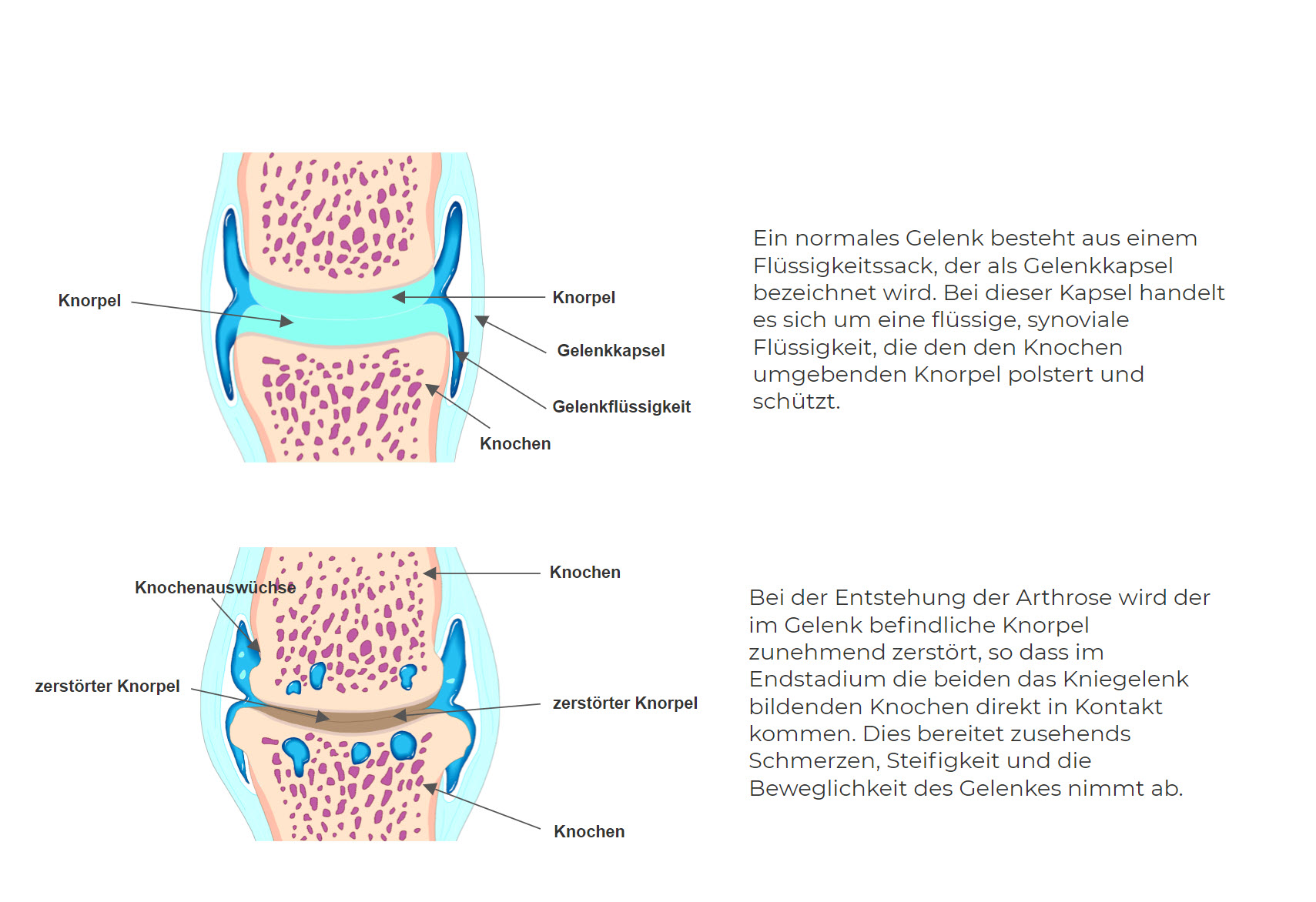
In general, we speak of arthrosis when the cartilage in a joint increasingly degenerates. Arthrosis is therefore also called joint wear. In knee arthrosis, the cartilage in the knee breaks down more and more. This in turn can cause changes in the adjacent bone. In this case, complaints such as pain, a feeling of stiffness and restricted movement occur, which increase over time.
How does osteoarthritis develop?
Cartilage can wear out with age or heavy use, because it constantly cushions movements and is exposed to friction from the bones. In principle, the body has a built-in protective mechanism for this: To compensate for damage, the joint cartilage can slowly renew itself. In osteoarthritis, however, the cartilage can no longer regenerate sufficiently on its own. There is increasing wear and tear of joint cartilage. Over time, this wear and tear can also spread to the tissues surrounding the cartilage.
Symptoms & complaints
Knee osteoarthritis is a disease that often begins insidiously. Its signs are hardly noticed at first.

Causes
There are influenceable and non-influenceable risk factors for the occurrence of knee osteoarthritis. They also apply to osteoarthritis in general. In all people, the joint cartilage wears out somewhat in the course of life. However, certain influences can accelerate the wear and tear and thus promote knee osteoarthritis.
Influenceable risk factors:
- Physical inactivity
- Heavy physical work (for example, kneeling occupations or performing heavy lifting work)
- Sport that puts a strain on the joints (for example, due to meniscus damage, a tear of the anterior cruciate ligament, a dislocation of the kneecap or a bone fracture near the knee joint.
- Overweight (People who have a body mass index (BMI) above 30 are considered to be severely overweight (obese). The higher the BMI, the greater the strain on the joints).
- Congenital or acquired deformities such as knock knees and bow legs
- Overloads and incorrect loads (accidental or congenital)
Risk factors that cannot be influenced:
- increasing age
- female sex
- Possibly genetic predisposition
Diagnosis
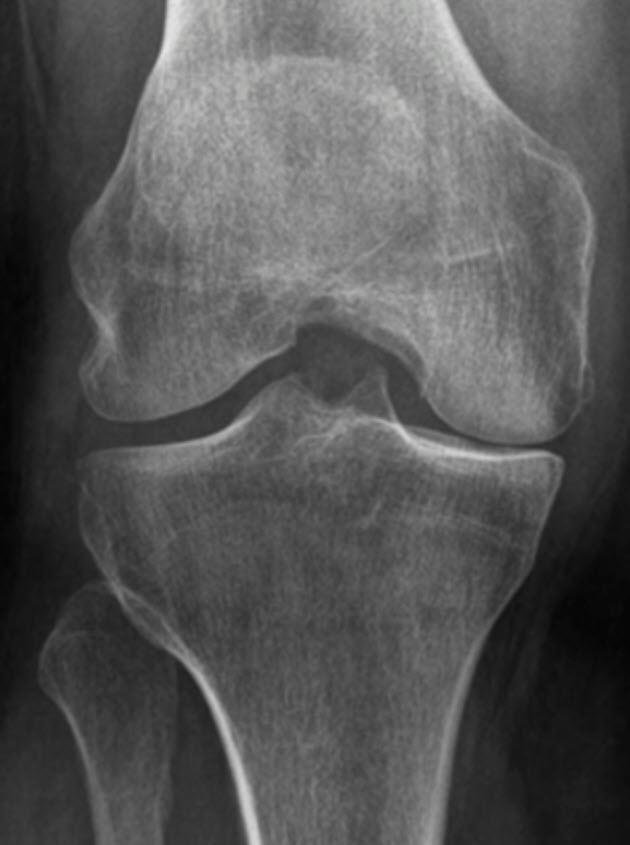
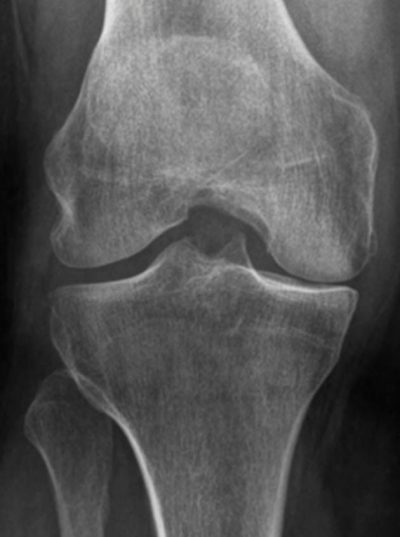
To diagnose knee osteoarthritis, a detailed history is first taken, with questions about symptoms such as recurrent or persistent pain and temporary stiffness in the knee. The examination as an obligatory medical activity assesses the range of motion of the knee joint, looks at the leg position and checks whether there are other possible causes for the pain, such as damage to the meniscus or the ligaments. Usually, an X-ray of the knee joint is enough to detect osteoarthritis. More specialised examinations, such as an X-ray of the whole leg, a computer tomography (CT) or a magnetic resonance imaging (MRI) are reserved for differential diagnostic questions in case of unclear findings. If the diagnosis is confirmed, regular X-ray checks are not necessary.
Treatment is based on the symptoms anyway and not on what can be seen on X-rays.
Types of knee osteoarthritis depending on the location of the cartilage defect:
- medial knee osteoarthritis: This type of knee osteoarthritis affects the inner (medial) part of the knee joint, primarily in bow-leg malalignments (varus gonarthrosis)
- Lateral knee arthrosis: This form of arthrosis is often associated with an X-B adjustment; the outer area of the knee is affected in particular (valgus gonarthrosis).
- retropatellar osteoarthritis: oste oarthritis behind the patella (kneecap) affects the joint between the kneecap and the thigh bone. (femoropatellar osteoarthritis).
- Pangonarthrosis: In pangonarthrosis, all compartments of the knee joint are affected. This means that the joint surfaces of the femur (thigh bone), the tibia (shin bone) and the patella are involved.
Treatment
Various therapy components can be considered for the treatment of osteoarthritis. Which ones are used depends, among other things, on how severe the pain and suffering of the affected person are and whether the mobility of the joint is impaired. Last but not least, the age of the patient also plays a role, as does the question of athletic ambition. Knee osteoarthritis typically begins with knee pain that initially occurs only with exertion. As it progresses over time, the pain becomes more frequent and severe. They can then also occur at rest or at night and disturb sleep.
Conservative treatment
Basically, the treatment of osteoarthritis aims to relieve or improve the pain, to maintain the mobility and resilience of the knee joint as long as possible and to continue the sporting habits relatively pain-free.
The following therapies are possible:
- Drug treatment: Drug therapy aims to relieve the pain or make it disappear completely. Oral anti-inflammatory painkillers such as diclofenac, ibuprofen and etoricoxib can relieve osteoarthritis pain. Paracetamol is not effective for knee osteoarthritis. Opioids often do not help better than anti-inflammatory pain relievers, but they have more side effects and can be addictive.
- Physical Therapy: Physiotherapy- Specific exercises to strengthen muscles and mobilize, leg axis training, improve pelvic and trunk stability.Many studies show that regular strengthening and flexibility exercises can relieve pain and improve joint function.
- Injection treatments with hyaluronic acid and regenerative cell therapy
- Physical measures: e.g. electrotherapy , cold treatment
- Aids: Shoe insoles, orthoses and relief shoes are low-risk options. However, their effect has not been well researched to date. In one conclusive study, a relief shoe did not alleviate knee pain any better than normal, well-fitting and cushioning shoes over several months.e. walking aids, knee supports, orthoses
- With X-ray stimulation radiation (also: orthovolt therapy), the joint is treated with weak X-rays 6 to 12 times over several weeks. There are no comparative studies on this treatment to date. It is therefore unclear whether it helps.
- Radiosynoviorthesis (RSO) involves injecting a low-level radioactive substance into the knee joint. A benefit has not been proven by studies, and there are also reports of complications such as bone and joint inflammation.
Surgical treatment
If the conservative treatment does not result in an improvement of the pain and the continued restriction of movement and stress, surgical treatment of the arthrosis is an option.
The following surgical procedures are available:
- Straightening (osteotomy) of O and/or X legs (varus-valgus gonarthrosis)
- Hemislide prostheses (unicondylar sled prosthesis)
- Total knee endoprosthesis (knee TEP)
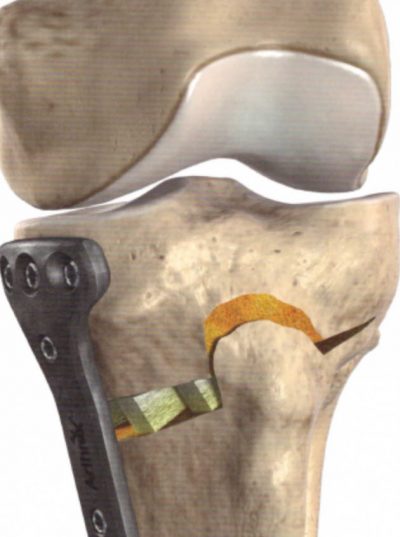
Straightening of the axis (conversion osteotomy)
Increased wear of the cartilage (osteoarthritis) on the inside or outside of the knee can be caused by an existing leg axis malposition. Meniscus (partial) removal can also lead to increased wear of part of the joint, resulting in a malalignment with osteoarthritis. O-legs (varus gonarthrosis) or X-legs (valgus gonarthrosis) can also be caused indirectly by an oblique fracture healing of a long bone in the upper or lower leg. This form of arthrosis in the knee occurs especially in X-B setting. Here, it is mainly the outer area of the knee that is affected.
Hemislide prostheses (unicondylar sled prosthesis)
This is a partial replacement of the knee joint. In this smallest and simplest version of an artificial knee joint, only the surfaces of the joint are replaced. It is used when the wear and tear on the knee joint is only one-sided and all the ligaments are still intact, for example in the case of one-sided wear and tear of the knee joint cartilage, as can occur with bow legs. Specifically, the joint surface at the bottom of the thigh is replaced with a prosthesis or crowned with a surface replacement, either the inner or outer part of the knee joint. On the tibia, only the joint surface opposite the prosthesis is replaced.

Knee TEP (total endoprosthesis)
In the advanced stage of cartilage destruction, several parts of the joint are usually affected. The knee joint becomes deformed and increasingly stiff. Patients suffer from pain on exertion and at rest, and some also experience pain at night. The pain-free walking distance becomes increasingly shorter and the quality of life is increasingly limited. X-rays show destroyed joint surfaces with visible joint deformities.


Aftercare
More information will follow shortly.
FAQs
More information will follow shortly.

